Intraosseous infusion
Intraosseous infusion is the process of injecting a solution into the bone marrow. The method is used in an emergency situation or when the traditional method of infusion is not possible, for example, if it is difficult to find veins due to massive blood loss. The input node can be used for no longer than 24 hours, otherwise there is a risk of infection in the bone.
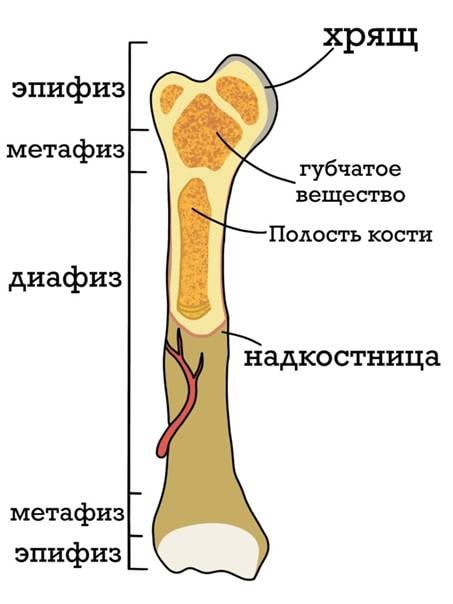
The bone marrow makes up about 4,5–4,7% of the body weight of an adult, about half of this mass is in the red bone marrow, located in the spongy substance of flat bones, vertebral bodies, metaphyses (the name of the bone department adjacent to the epiphasic line left over from the cartilaginous growth plates) of tubular bones.
Red bone marrow consists of myeloid tissue, which is a type of connective tissue, with vessels located in it, and is the main organ of hematopoiesis, providing not only the formation of all types of blood cells, but also delivering stem cells to other organs and tissues. From stem cells, erythrocytes, all types of granulocytes, platelets, monocytes and lymphocytes are formed.
The red bone marrow is a self-regulating system. It controls the body's need for certain cells and controls the intensity of their formation. This regulation is provided by a complex set of nervous, humoral, biochemical and other mechanisms.
The discovery in the 1920s of the properties of the bone marrow to conduct the administered drugs affected primarily pediatric resuscitation. Soviet scientists in the course of morphological and histological studies in the period from 1940 to 1950 substantiated and introduced the practice of not only intraosseous administration of drugs, but also intraosseous anesthesia. The pathways of anesthetic outflow from the bone were studied in detail, and it was shown that the drug solution injected into the bone marrow evenly infiltrates the surrounding soft tissues.
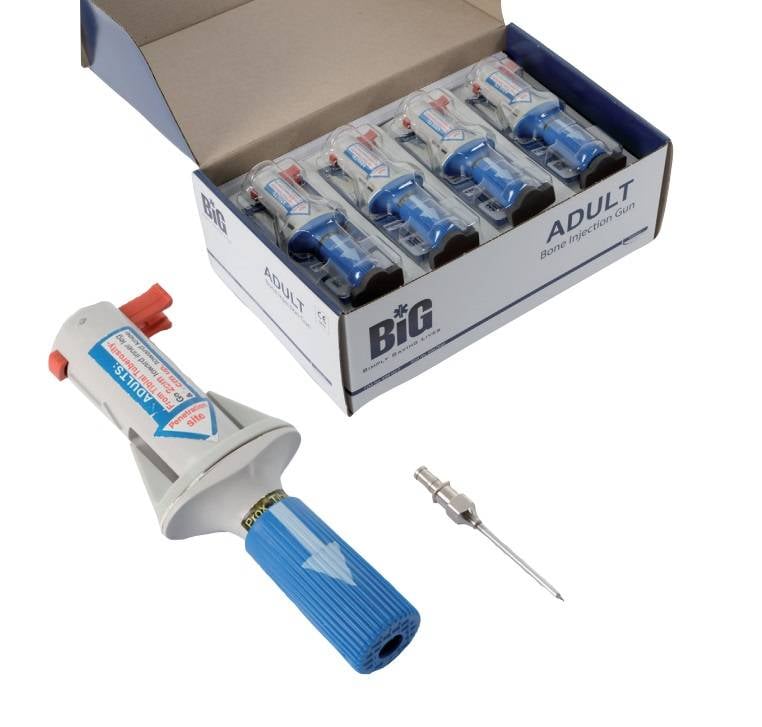
In the case of syringe guns, children and adults are distinguished, which is very important due to the difference in the thickness of the needle and the pulse device, which ensures that the needle is inserted to the desired depth. Nowadays, most often you can find a syringe gun for intraosseous injection BIG (Bone Injection Gun) made in Israel. Red is for children, blue is for adults.

Setting up an IV in adults in a moving ambulance can take 10–12 min, with a 10–40% failure rate. A study of intravenous access attempts in pediatric practice by ambulance workers showed that more than one-third of the attempts to complete the procedure took more than 5 minutes, and in one quarter of the cases, more than 10 minutes. In 6% of the attempts it was completely impossible to obtain intravenous access. At the same time, with intraosseous access in pediatric and adult patients, in 70-100% of cases it was possible to achieve success within one minute.
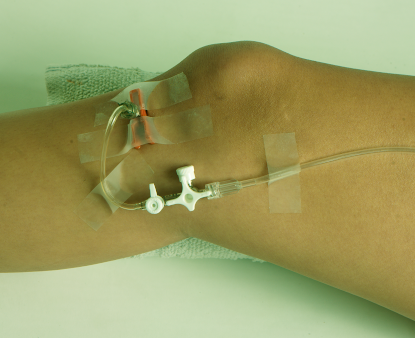
For adults, intraosseous access is placed in the sternum or tibia. In addition, the radius and ulna, pelvis, clavicle, calcaneus can be used. The choice of location depends on the presence of fractures or upcoming procedures.
When installing a bone access, the needle pierces the outer hard part of the bone with a characteristic click and is securely fixed by the bone cortex in a given position. In some cases, when the trocar stylet is removed, bone marrow can enter the needle cannula. Yes, it sounds and looks not very good, but nothing fatal happens. In fact, a trocar is an extremely interesting device, invented at the beginning of the XNUMXth century, for penetration into cavities while maintaining tightness. Decompression needles work in a similar way.

The most common complication of intraosseous infusion under non-sterile conditions is infection or osteomyelitis. In addition, unrecognized infiltration can lead to local necrosis. For this reason, once an access has been established, the surrounding tissues should be checked regularly for infiltration, as with traditional intravenous infusion. If it is detected, the infusion should be stopped immediately.
If an intraosseous access device has been unsuccessfully inserted or removed, retrying or placing a new device in the same bone is prohibited.
In general, intraosseous injection is just a quick response in emergency situations and is not a substitute for classic intravenous infusion. There is no special qualitative difference between them. You can enter the same drugs, and their delivery takes approximately the same time.
Conclusions
First of all, it must be understood that for an ordinary person without specialized knowledge, the availability of tools for intraosseous injection is useless. This applies equally to decompression needles or non-valve occlusive dressings, as well as any other specific assistive devices.
However, given the ongoing hostilities and the trend of their development, the need for such funds may increase. In 2018, the journal "Bulletin of the Russian Military Medical Academy" published research results prototypes on a mechanical and electric drive. Based on the results, medical devices were recommended for inclusion in the standard equipment and for supplying the medical service of the Armed Forces of the Russian Federation.
At present, I have not been able to find analogues of the Bone Injection Gun of our production. Perhaps, of course, there is no need for them, although, in my opinion, not a single ambulance resuscitation team, not to mention military doctors, will refuse such a compact and effective device, but something else worries: what if they are needed, but against the background of mobilization and universal dronophilia just forgot about them?
Information