Why are Russians dying out?
Necessary foreword
I present to your attention a material in which the main part of the work was done by our reader. I represent him as Dr. Watson, since the research was really done at the highest level, but since the person is directly related to the subject of discussion, then you should not look for adventure. Today in our country this is sometimes fraught.
So I confirm the truth of the materials and conclusions and recommend that you do not take this to heart, but just think about the situation.
Roman Skomorokhov

To start when everything is sad, in principle, it doesn’t matter where, because everywhere we have health plans, to put it mildly, not really. We decided to start with the most topical, namely, with such a thing as life expectancy - Life expectancy.
Agree, this is important. Moreover, it is important for every resident, regardless of age, gender and other things. We all want to live as long as possible and not do anything about it. That is the nature of man.
And we will compare this parameter not only with the countries of the "old world", but take into consideration those who used to be either one with us or who were in a political and economic cage.
This is the so-called "new eight" of the EU countries, Hungary, Latvia, Lithuania, Poland, Slovakia, Slovenia, the Czech Republic and Estonia.
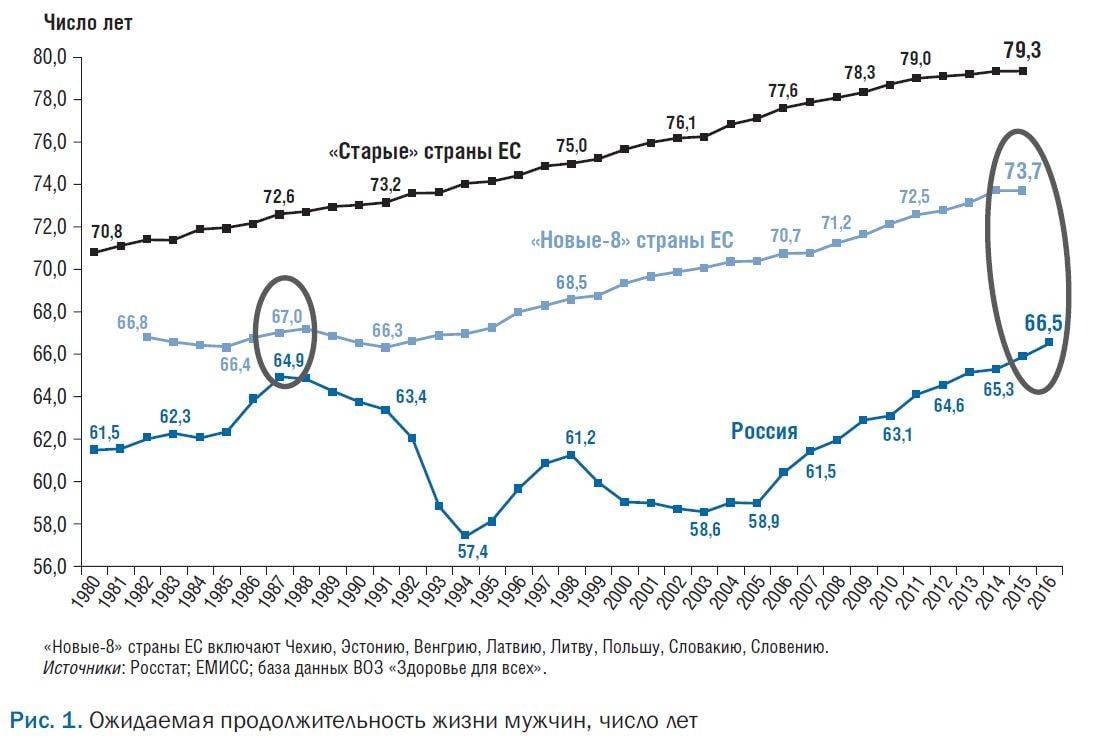
Today, life expectancy in Russia is by 6 years lower than in the "new-8" EU countries that have a level of economic development close to the Russian Federation, and in 1987, this difference was less than 1 of the year.
1-I and the biggest problem - the high mortality of citizens of working age. It is 3,4 times higher per 100 thousand population than in EU countries.
High mortality rates for men lead to the fact that the life expectancy of Russian men is 10,6 less than Russian women and 7 less than the life expectancy of men in the “new-8” EU countries.
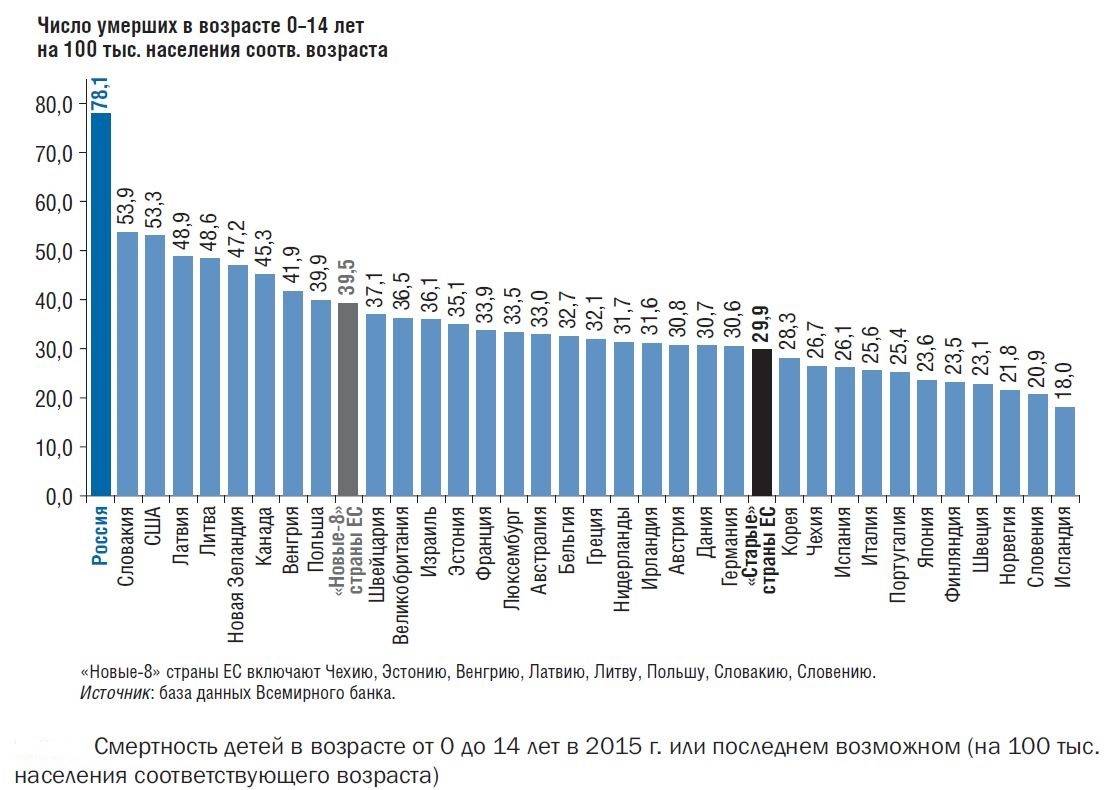
The 2 problem is the health of Russian children, mortality among them is 2 times higher than in the “new-8” EU countries (see the chart below), especially between the ages of 1 and 14 years. Moreover, half of the deaths at this age occur as a result of external causes (!) (43%) and neoplasms (!) (12%).
3-I problem - high mortality from neoplasms among young ages. Thus, the standardized mortality rate (SCS) of men under the age of 65 years from malignant neoplasms in the Russian Federation is 1,5 times higher than in the EU countries, and the SCS of women is 20% higher.
4-I - extremely unsatisfactory mortality rates from infectious diseases. SCS from them is 4 times higher than in the "new-8" EU countries, and from tuberculosis - 8 times higher (SCS is calculated according to the world standard).
Moreover, mortality from infectious diseases over the past 4 years (from 2012 to 2016) has increased by 8%. Moreover, this growth occurred due to deaths from HIV - in 2 times and from viral hepatitis - in 1,4 times.
5-i problem - a significant difference in health status between rural and urban residents. In the village they live on 1,9 less than in the city.
In 1995 (This is the dashing 90!), This difference was almost 3 times lower and amounted to only 0,7 of the year. Those. Today, the difference in health status between rural and urban residents (read, the difference in material well-being) has grown by almost 1995 times compared to 3!
And this difference continues to grow, unless, of course, we are talking about such prosperous regions in this regard as the territories of the North Caucasus that are part of the Russian Federation, where, according to sociological research, today, compared to previous periods, an unprecedented increase life expectancy and its quality, the general state of health of the indigenous population, combined with a reduction in mortality.
In 2016, government healthcare spending in the Russian Federation amounted to 3,1 trillion rubles, or 3,6% of GDP. In the "new-8" EU countries, this share is 1,4 times higher - 5,0% of GDP.
But money is far from everything, although, of course, finances decide a lot. Insufficient resource provision of Russian healthcare is compounded by inefficient management.
Ineffective management is manifested in the fact that:
- the industry has not identified priorities;
- there is a contradictory regulatory framework,
- the regulatory requirements themselves are often not provided with the necessary resources;
- statistics are inconsistent or closed;
- an objective system analysis of the activity is not carried out, as a result, the correct decisions are not made;
- requirements of mandatory procedures are not consistent with methodological documents,
attached to the State Guarantees Program.
- the requirements of medical care standards and procedures for its provision are often
not provided with resources, and therefore not feasible.
At the same time, numerous inspections of control and oversight bodies are carried out for compliance with the requirements of orders and standards, but the effectiveness of these inspections is a big question.
Moreover, the control measures themselves and the criteria for inspections are multiplying, the reported workload of medical personnel reaches 70% of working time (in places up to 90%).
So, in the order of the Ministry of Health of Russia from 10.05.2017 No. 203н “On the approval of the criteria for assessing the quality of medical care” about 2400 indicators are defined.
In developed countries, no more than 30 – 50 result indicators are usually used to control medical organizations.
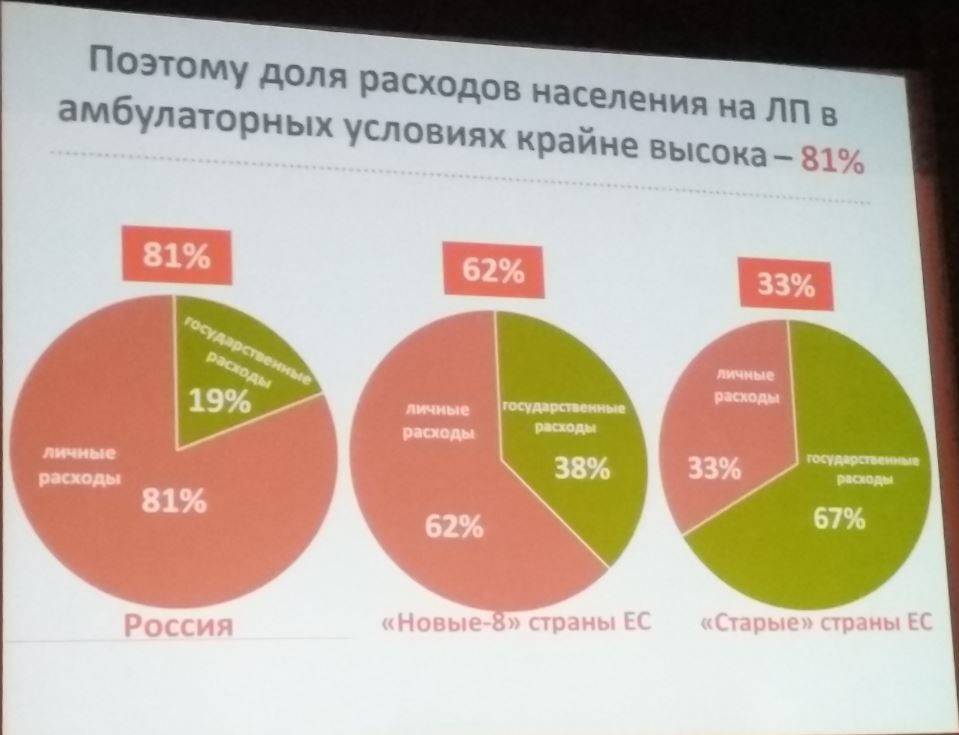
RF free drug provision is available only to certain categories of citizens; in addition, it is 2,4 times lower in per capita expenditure than in the “new-8” EU countries and 4,4 times lower than in the “old” EU countries.

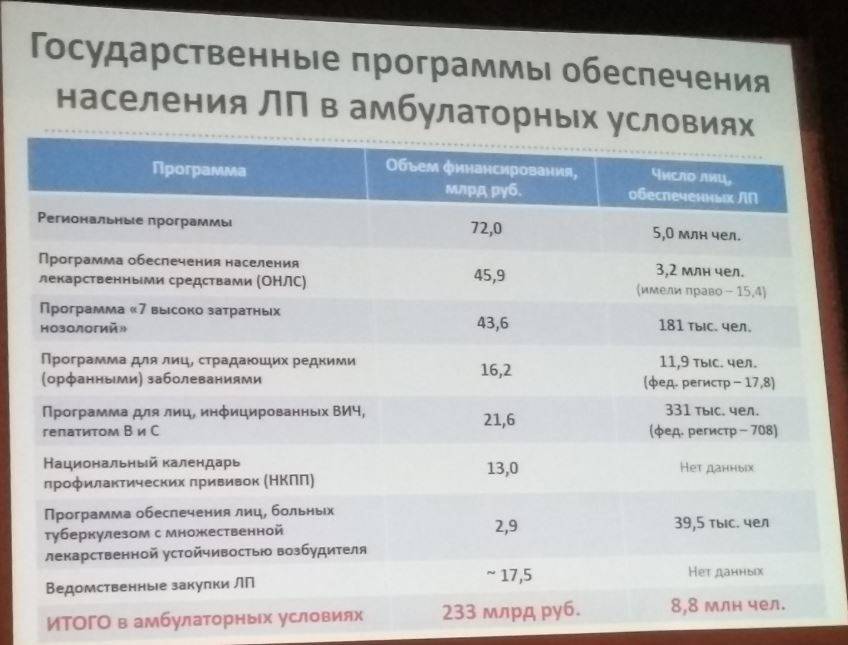
Respectively:
But, at the same time:
This, in fact, is obtained?
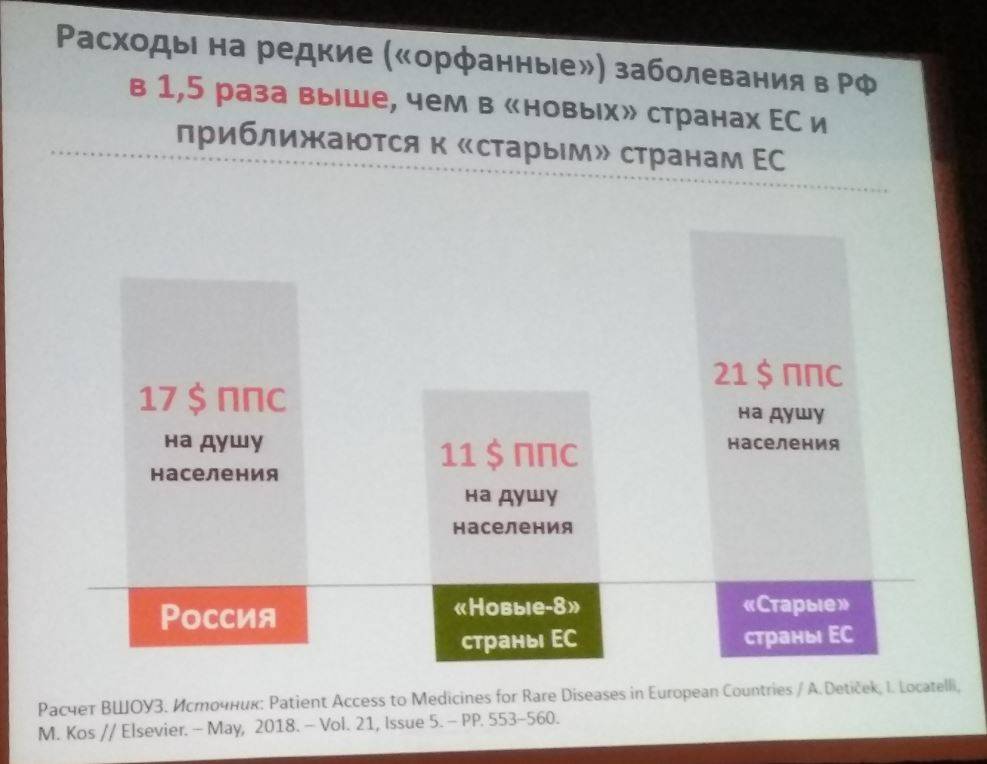
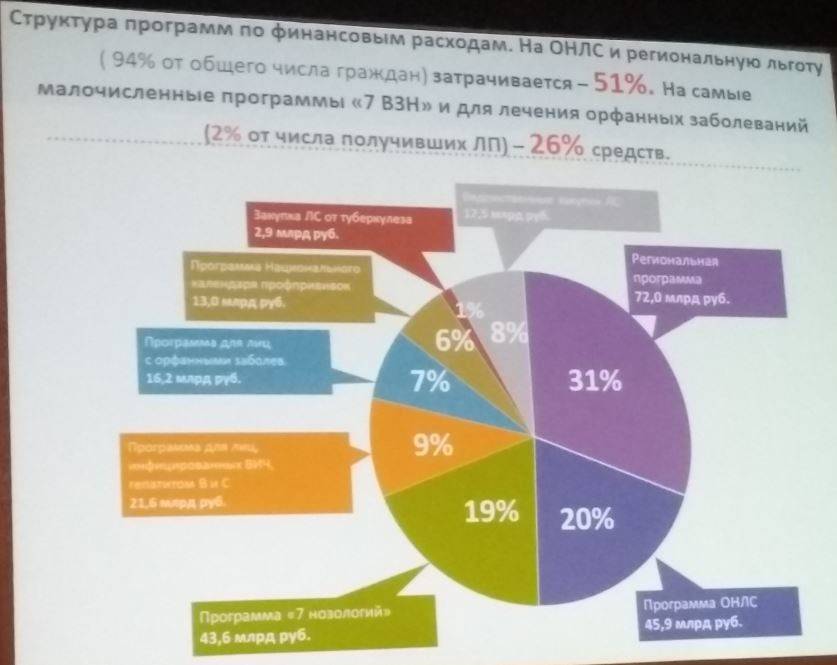
The country is pouring enormous amounts of money into a bottomless barrel of orphan pathology and 7 VZN without any hope for this country to receive at least some return on these inferior children in the future and, at the same time, refuses the slightest adequate medical and medical support for people on which the welfare of this country rests!
We spend enormous amounts of money on hopeless people in terms of recovery and future “return”, and we are not going to cut these budgets, while in the country the retirement age rises by 5 years due to the fact that the budget is being overloaded by paying pensions to people who in all respects they deserve it!
Is this what is actually happening in our country?
From 2012 to 2016, as a result of “deeply thought out” reforms by our government, the capacity of the state healthcare system was reduced and, as a result, its throughput decreased, i.e. the ability to provide free medical care has actually decreased.
All this had an extremely negative effect on the process of interaction between patients and doctors, while the latter became hostages of “strictly faithful government” decisions.
Over the same period (2012 - 2016 gg.), The number of patients in the Russian Federation increased by 2% (+ 4,2 million people), and the availability of doctors decreased by 4%. And this despite the fact that already in 2012, the majority of Russian doctors worked with significant overload (the combination factor was at least 1,5).
As a result, the availability of doctors in the Russian Federation today has been established at the level of the EU countries, and this with a large flow of patients and significantly greater distances.
Provision of stationary beds for 2012 – 2016 in Russia also decreased by 13%. As a result, the number of visits to outpatient facilities (by 12%) and hospitalizations (by 13%) decreased.
As a result of "optimization", many FAPs (feldsher-midwife centers), rural precinct and district hospitals, and maternity hospitals were closed.
But in a significant number of perinatal centers have been built and continue to be built.
Has anyone explained to the president’s friends, his guards and other persons close to him or his friends who are in power today, what are they for and what is the perinatal period for?
In Japan, for example, they began to create perinatal centers only when they solved the visible problems of obstetric care and the removable causes of maternal and infant mortality.
Only after that they dealt with more subtle problems at the mother-fetus level, for which perinatal centers were needed.
As a result of the carried out "optimization" 25,8% of the inhabitants of our country, i.e. rural residents and the population in small towns were left without affordable and high-quality medical care.
The share of rural district hospitals accounted for 47% of all hospital admissions in the country, and the FAPs and rural outpatient clinics accounted for 53% of all visits, i.e. liquidated the most massive medical institutions, and this mass cannot be restored.
Of the 4500 rural district hospitals throughout the country, only 400 (!!!) remained.
A targeted and at the same time galloping reduction of the most functional element of primary health care (PHC) more than 10 times!
As a result of "optimization", it is often necessary even to get to the paramedic for 30 – 40 km, but not everyone can. Due to the considerable distances (the country is huge) and the condition of local roads (136 place from 144 countries), medical assistance is virtually unavailable for the village, small towns and settlements. And all the achievements of medicine are concentrated in large cities and in medical centers.
Now, by the number of hospitals, we are rapidly approaching the 30 years of the last century.
Are we as healthy as a nation? You can think so, if you do not go to the district hospital for years. Or never try to make an appointment with a specialist doctor.
And this is our New Russia, which we seem to be building together (the president said, if that) we are building ...
What would a prudent landowner do when moving to new housing? I mean, you understand, moving from the USSR to Russia.
He would take from the past all the most valuable and useful, and he would get rid of the negative.
Well-organized sanitary aviationemergency medical service with an approved list of emergency conditions, a system of continuing medical education, two- and three-link systems, preliminary rooms, geriatric rooms in clinics, etc.?
And where did the Pirogov system of staged medical care with patient routing, which formed the basis of the military medical doctrine, leading to the greatest exit into the system, disappear?
If earlier the doctor not only interviewed, examined, auscultated, palpated and percussed his patients, talked with them, but he could also hypothesize the disease (hemorrhoids, arthrosis, etc.) by walking in a long office, but now the doctor is not up to the patient , since based on his complaints he must correctly fill out the documentation on the computer (otherwise there may be fines) or send the patient further for examination and consultation. Paid, often.
It's a shame to say, but only now and only in Moscow will doctors be taught how to communicate with patients!
In addition to all of the above, health problems are also associated with the compulsory health insurance system, when state money is sent to state medical organizations (and such 96%) through private commercial insurance medical organizations (SMOs), the main purpose of which, as it’s not disguised, is not to help patients , and making a profit, including by imposing penalties on medical institutions, finding fault with errors in filling out documents.
In other words, QS inspectors are economically interested in poor-quality work of medical organizations.
And the MHI system itself is becoming obsolete, even in Germany, which follows from the websites of the Bundestag deputies, since the increase in contributions lags far behind the needs of the population, especially older people, whose number is growing, but you can’t count on migrants.
Moreover, all participants in the compulsory medical insurance are economically interested in increasing the number of medical services, in treating, but not curing, in increasing the number of patients, although the interests of the state should be directly opposite.
Today, countries with health insurance demonstrate much lower efficiency (in terms of cost-performance ratio) of healthcare than countries with a state-budget model (Britain, Spain, Italy, Denmark, Sweden, Norway, Finland, Canada, Australia, etc.).
Private commercial clinics, although they are part of the national healthcare system under the Constitution of the Russian Federation, do not save the situation, because at any time they can be transformed, re-profiled, closed, etc. therefore, they should not be dominant, but only complementary, substitute and competing with respect to state clinics.
Only 1 / 5 part of the country's population can partially use paid services in public and private clinics, since the gap in incomes and opportunities between the rich and the poor is only widening.
Citizens ’payments are also not an option, because people get the necessary medical care at the right time and pay taxes and receive part of their wages, so the result will be a radical increase in their dissatisfaction with the powerlessness of the authorities to plan budget expenses correctly taking into account priorities.
At the same time, today, only according to official statistics, our citizens already pay 35% of healthcare spending. But this is the "official" statistics, in fact, of course, more.
Based on the foregoing, the first thing that should be done immediately is to separate the health insurance system from the compulsory health insurance system and instruct them to develop the embryonic VHI sector, and the function of insurers should be allocated to the territorial compulsory health insurance, making them branches of the federal compulsory health insurance system - the only insurer in the whole country.
This, with the appropriate political will, would make it possible to find time for the preparation and implementation of the necessary transformations.
All over the world they try not to bring patients to expensive high technologies, but to solve their problems earlier, at earlier stages.
But we have more and more neglected, missed and severe cases of diseases.
In 2012, in order to heroically solve this purposefully created problem, the national expert community, represented by specialists from the Ministry of Health of the Russian Federation, the MHIF and World Bank staff (where without them), began to develop a Russian model of clinical and statistical groups (CSG) of diseases.
As always, the regions participating in the pilot project reported on the exceptional economic success of the program over the past 5-year period (2014-2018):
“Over the past 5 years, the average length of a patient’s stay in a hospital bed decreased by 1,5 days, daytime by more than 2. There was a natural optimization (again, optimization, what a sweet word!) Of medical organizations in general and hospital beds in particular. The changed medical network now more closely matches not the historical, but the real needs of the population in the volumes and structure of the medical care provided. ”
Here it turns out, like, in spite of everything, according to the report of the leadership of the TFOMS of the Sverdlovsk region and the head of the department of the Ural Federal University named after First President of Russia B.N. Yeltsin »the current medical network now optimally meets the real needs of the population in the volume and structure of the medical care provided!
Compare the above quote with the data and stated problems that are presented at the beginning of this article.
Although, indeed, tactically certain successes have certainly been achieved.
In the Sverdlovsk Region in 2014, hip joint replacement operations began to be paid with the 4,5 coefficient, while the federal directory recommended the 1,92 weight coefficient.
This decision, coupled with the immersion of several types of high-tech medical care of this profile in the compulsory medical insurance system, increased the availability of modern surgical care using osteosynthesis for the population and became one of the reasons for the complete elimination of the line for hip arthroplasty in the Sverdlovsk region in 2015. Innovations in payment have led to an increase in the number of slightly traumatic arthroscopic interventions, osteosynthesis using modern titanium metal structures.
But strategically, the implementation of this model in the same Sverdlovsk region led to the following:
Routing of patients, changing the structure of medical care in favor of increasing the share of costly specialized medical care (the need for which is purposefully potentiated by eliminating the primary care unit (see above.)) Caused (apparently, as intended) a natural outflow of funds from medical organizations I level.
If in 2014 the amount of funds earned by round-the-clock level I hospitals exceeded 29% of the total funding for specialized care, in 2017 its share decreased to less than 25%. Accordingly, funding for around-the-clock hospitals at levels II and III increased.

A similar, but even more revealing picture began to be observed in the day hospital. Over the 4 of the year, the volume of funding for hospital-replacing care in level I medical facilities decreased from 40 to 26%. This is due to the provision of the most expensive care, including chemotherapy and dialysis, at levels II and III.

That is, let's build expensive dialysis centers and then, of course, give them to private hands (for example, the vast majority of dialysis centers in the Russian Federation are under the patronage of the Fresenius company. EUROMEDICA is the company to build its dialysis centers, which were later transferred to Fresenius). (the Israeli beneficiary) received money from the budgets of the respective regions), and then we will allocate very considerable amounts from the same budget for dialysis and concomitant therapy.
And this is instead of trying to the maximum extent possible to suppress the factors contributing to the development of terminal chronic renal failure, with all the positive social and economic consequences for the population and the country as a whole.
Further, according to the report of the same persons from the leadership of TFOMS of the Sverdlovsk region and the Federal State Autonomous Educational Institution of Higher Education “Ural Federal University named after First President of Russia B.N. Yeltsin, ”it turns out,“ the financial difficulties that level I hospitals are experiencing for objective reasons are exacerbated by their inefficient costs, which are primarily associated with excessive staffing, excess space, and bed capacity.
So they sailed. The circle is closed (see the beginning of the article).
It turns out that despite the shortage of beds, the real problems with staff in the primary care, we need further optimization in addition to the one that has already been carried out and whose errors are blamed at all angles, and its results in the solid residue are given at the beginning of this material.
It turns out that under the guise of KSG and statements about local dizzying successes, under the guise of and with the highest permission, the systematic destruction of the country's real health care system continues with parallel pumping of budget money into all possible private pockets.
The issue of today's healthcare organization is generally a separate issue.
The main problem is not in the level of development of clinical medicine and its capabilities, but in the normal organization of medical care.
According to the paradigm imposed on society, it is believed that every doctor can be the organizer of health care.
Approximately the same kind of people in our country are versed in football, but coaches are specially trained.
For full-fledged work on the organization of healthcare, common sense, personal devotion, family or friendships are not enough, at least special and different knowledge is still needed:
- to the head physician - how to organize the interaction of all services, how to ensure quality, efficiency, how to evaluate activity correctly, and for this it is necessary to attract market mechanisms, etc .;
- the territorial leader needs knowledge about the interaction of various organizations, about the stages of medical care and patient routing, about the methodology for drawing up strategies, concepts, programs and projects, as well as the ability to correctly analyze and evaluate work, etc.
And here the results should not be indicators of public health, but the frequency of prevented cases of diseases, restoration (partial or complete) of lost health and disability for medical reasons.
Not a defeated disease, but a prevented one. Not the war won, but the created impossibility of war, as such.
Confucius rightly believed that causes are more important than results, and this is directly related to human diseases. More than 150 years ago N.I. Pirogov predicted that the future belongs to preventative medicine.
I wonder what time in relation to N.I. We live in Pirogov if in 2016 at the All-Russian Youth Educational Forum it was proclaimed that the main principle of the medicine of the future (again someday) is prevention.
Apparently, the many close to the authorities, occupying the posts of medical officials, it is very profitable to push this future for us all the time for later.
As far back as 1937, the famous American specialist and historian of medicine Henry Sigerist wrote that the era of the millennial dominance of medical medicine is ending, the era of preventive medicine is coming, the foundations of which appeared in the USSR. Even the famous scientist Claude Bernard believed that every doctor should know 3 things:
- health conditions to support them,
- conditions for the development of diseases in order to prevent them,
- conditions of recovery to use them.
Today, the population in Russia in all possible ways makes us forget that doctors should deal not only with treatment, but also with the causes of diseases and the factors affecting them.
Of course, medical medicine has not yet exhausted itself, and its technological capabilities require wider distribution, and not concentration only in large clinics. And for some time, medical medicine can be combined with preventive medicine, but this must be seriously addressed.
The organization of health care is closely connected with the policy pursued, with the socio-political and economic model that is being created in the country.
What kind of final model is being created in our country for a wide circle of people is not known, the president publicly prefers not to talk about which country we are building, but puts forward immediate and remote tasks.
What the immediate and remote tasks of the country’s population and, possibly, in the future, its territorial integrity are, one can only guess, but if a school, FAP or rural dispensary are closed in the village, the village dies without these centers of culture, and, therefore, the lands around are overgrown with thistles. And today, to a greater extent than ever before, starting from the 90's, this trend can be justifiably extrapolated to the entire Russian Federation, with the exception of probably the happiest individual regions with rapidly improving duration and quality indigenous life.
Already now in Russia 13% of rural settlements have no residents at all.
And it will be very interesting to trace who already owns these lands, or who will become their owner in the near future, what will happen in these territories and whose interests it will serve. But, at the moment, it goes beyond the narrow scope of the topic that this article is intended to cover, and is the subject of a separate painstaking and, most likely, very unsafe study.
Unfortunately, according to the results of the analysis of the situation in the healthcare system of the Russian Federation, the conclusions regarding the socio-political model that our country is being imposed on are quite not in favor of the president, government and the existing vertical of power, and, most sadly, not in favor of prospects the existence of primarily the Russian people!
That is, following this path, we, as a people, can only come to one place: on historical cemetery. Near the Parthians, Polovtsy, Bulgars and others. It's a shame, but it's true today.
According to the materials of the Bulletin of the Higher School of Health Management Organization (HSE) and the FS data on supervision in the field of consumer protection and human well-being (Rospotrebnadzor).
Information